How do healthcare professionals in a chiropractic clinic provide a clinical approach to preventing medical errors for individuals in pain?
Муқаддима
Medical errors resulted in 44,000–98,000 hospitalized American deaths annually, and many more caused catastrophic injuries. (Kohn et al., 2000) This was more than the number of people who died annually from AIDS, breast cancer, and auto accidents at the time. According to later research, the actual number of deaths may be closer to 400,000, placing medical errors as the third most common cause of death in the US. Frequently, these mistakes are not the product of medical professionals who are inherently bad; rather, they are the outcome of systemic issues with the health care system, such as inconsistent provider practice patterns, disjointed insurance networks, underutilization or absence of safety protocols, and uncoordinated care. Today’s article looks at the clinical approach to preventing a medical error in a clinical setting. We discuss associated medical providers specializing in various pretreatments to aid individuals suffering from chronic issues. We also guide our patients by allowing them to ask their associated medical providers very important and intricate questions. Dr. Alex Jimenez, DC, only utilizes this information as an educational service. Радди
Defining Medical Errors
Determining what medical error is the most crucial step in any conversation about preventing medical errors. You might assume this is a very easy chore, but that is only until you delve into the vast array of terminology utilized. Many terms are used synonymously (sometimes mistakenly) since some terminology is interchangeable, and occasionally, the meaning of a term depends on the specialty being discussed.
Even though the healthcare sector stated that patient safety and eliminating or reducing medical errors were priorities, Grober and Bohnen noted as recently as 2005 that they had fallen short in one crucial area: determining the definition of “perhaps the most fundamental question… What is a medical error? A medical error is a failure to complete a planned action in a medical setting. (Grober & Bohnen, 2005) However, none of the terms that one would often identify expressly with a medical error—patients, healthcare, or any other element—are mentioned in this description. Despite this, the definition offers a solid framework for further development. As you can see, that specific definition consists of two parts:
An execution error: A failure to complete a planned action as intended.
A planning error: is a technique that, even with perfect execution, does not produce the desired results.
The concepts of faults of execution and planning errors are insufficient if we are to define a medical error adequately. These may occur anywhere, not only at a medical establishment. The component of medical management must be added. This brings up the idea of unfavorable occurrences, known as adverse events. The most common definition of an adverse event is unintentional harm to patients brought about by medical therapy rather than their underlying disease. This definition has gained international acceptance in one way or another. For example, in Australia, the term incidents are defined as in which harm resulted in a person receiving health care. These consist of infections, injury-causing falls, and issues with prescription drugs and medical equipment. Certain unfavorable occurrences might be avoidable.
Common Types of Medical Errors
The only issue with this notion is that not all negative things happen accidentally or intentionally. Because the patient may ultimately benefit, an expected but tolerated adverse event may occur. During chemotherapy, nausea and hair loss are two examples. In this instance, refusing the recommended treatment would be the only sensible approach to prevent the unpleasant consequence. We thus arrive at the concept of preventable and non-preventable adverse occurrences as we further refine our definition. It isn’t easy to categorize a choice to tolerate one impact when it is determined that a favorable effect will occur simultaneously. But purpose alone isn’t necessarily an excuse. (Patient Safety Network, 2016, para.3) Another example of a planned mistake would be a right foot amputation due to a tumor on the left hand, which would be accepting a known and predicted unfavorable event in the hopes of a beneficial consequence where none has ever arisen before. There is no evidence to support the anticipation of a positive outcome.
Medical errors that cause harm to the patient are typically the focus of our research. Nonetheless, medical mistakes can and do occur when a patient is not harmed. The occurrence of near misses could provide invaluable data when planning how to reduce medical errors in a healthcare facility. Still, the frequency of these events compared to the frequency clinicians report them needs to be investigated. Near misses are medical errors that could have caused harm but did not to the patient, even if the patient is doing well. (Мартинес ва дигарон, 2017) Why would you acknowledge something that could potentially result in legal action? Consider the scenario where a nurse, for whatever reason, had just been looking at photographs of different medications and was about to provide a medication. Maybe something lingers in her memory, and she decides that’s not how a specific medication looks. Upon checking, she found that the incorrect medicines had been administered. After checking all the paperwork, she fixes the mistake and gives the patient the right prescription. Would it be possible to avoid an error in the future if the administration record included photographs of the proper medication? It is easy to forget that there was a mistake and a chance for harm. That fact remains true regardless of whether we were fortunate enough to find it in time or suffer any negative consequences.
Errors of Outcomes & Process
We need complete data to develop solutions that improve patient safety and decrease medical errors. At the very least, when the patient is in a medical facility, everything that can be done to prevent harm and put them in danger should be reported. Many doctors have determined that using the phrases errors and adverse events was more comprehensive and suitable after reviewing mistakes and adverse events in health care and discussing their strengths and weaknesses in 2003. This combined definition would increase data gathering, including mistakes, close calls, near misses, andactive and latent errors. Additionally, the term adverse events includes terms that usually imply patient harm, such as medical injury and iatrogenic injury. The only thing that remains is determining whether a review board is a suitable body to handle the separation of preventable and non-preventable adverse events.
A sentinel event is an occurrence where reporting to the Joint Commission is required. The Joint Commission states that a sentinel event is an unexpected occurrence involving a serious physical or psychological injury. (“Sentinel Events,” 2004, p.35) There isn’t a choice, as it needs to be documented. Most healthcare facilities, however, do keep their records outlining sentinel incidents and what to do in the event of one to guarantee that the Joint Commission standards are met. This is one of those situations when it’s better to be safe than sorry. Since “serious” is a relative concept, there may be some wriggle room when defending a coworker or an employer. On the other hand, reporting a sentinel event incorrectly is better than failing to report a sentinel event. Failing to disclose can have serious consequences, including career termination.
When considering medical errors, people frequently make the mistake of focusing just on prescription errors. Medication errors are undoubtedly frequent and involve many of the same procedural flaws as other medical errors. Breakdowns in communication, mistakes made during prescription or dispensing, and many other things are possible. But we would be gravely misjudging the issue if we assumed that drug errors are the only cause of harm to a patient. One major challenge in classifying the different medical errors is determining whether to classify the error based on the procedure involved or the consequence. It is acceptable to examine those classifications here, given numerous attempts have been made to develop working definitions that incorporate both the process and the outcome, many of which are based on Lucian Leape’s work from the 1990s.
Enhance Your Lifestyle Today- Video
Analyzing & Preventing Medical Errors
Operative and nonoperative were the two main categories of adverse events that Leape and his colleagues distinguished in this study. (Leape et al., 1991) Operative problems included wound infections, surgical failures, non-technical issues, late complications, and technical difficulties. Nonoperative: headings such as medication-related, misdiagnosed, mistreated, procedure-related, fall, fracture, postpartum, anesthesia-related, neonatal, and a catch-all heading of the system were included under this category of adverse occurrences. Leape also classified errors by pointing out the point of process breakdown. He also categorized these into five headings, which include:
система
Иҷрои
Муносибати маводи мухаддир
ташхис
Пешгирикунанда
Many process faults fall under more than one topic, yet they all help to pinpoint the exact cause of the issue. If more than one physician was engaged in determining the precise areas that need improvement, then additional questioning might be required.
Technically, a medical error can be made by any staff member at a hospital. It is not limited to medical professionals like physicians and nurses. An administrator may unlatch a door, or a cleaning crew member could leave a chemical within a child’s grasp. What matters more than the identity of the perpetrator of the mistake is the reason behind it. What before it? And how can we make sure that doesn’t occur again? After gathering all the above data and much more, it’s time to figure out how to prevent similar errors. As for sentinel events, the Joint Commission has mandated since 1997 that all of these incidents undergo a procedure called Root Cause Analysis (RCA). However, using this procedure for incidents that need to be reported to outside parties would need to be corrected.
What Is A Root Cause Analysis?
RCAs “captured the details as well as the big picture perspective.” They make evaluating systems easier, analyzing whether remedial action is necessary, and tracking trends. (Williams, 2001) What precisely is an RCA, though? By examining the events that led to the error, an RCA can focus on events and processes rather than reviewing or placing blame on specific people. (AHRQ,2017) This is why it is so crucial. An RCA frequently makes use of a tool called the Five Whys. This is the process of continuously asking yourself “why” after you believe you have determined the cause of an issue.
The reason it’s called the “five whys” is because, while five is an excellent starting point, you should always question why until you identify the underlying cause of the problem. Asking why repeatedly could reveal many process faults at different stages, but you should keep asking why about every aspect of the issue until you run out of other things that could be adjusted to provide a desirable result. However, different tools besides this one can be utilized in a root cause investigation. Numerous others exist. RCAs must be multidisciplinary and consistent and involve all parties involved in the error to avoid misunderstandings or inaccurate reporting of occurrences.
хулоса
Medical errors in healthcare institutions are frequent and mostly unreported events that seriously threaten patients’ health. Up to a quarter of a million individuals are thought to pass away each year as a result of medical blunders. These statistics are unacceptable in a time when patient safety is supposedly the top priority, but not much is being done to alter practices. If medical errors are accurately defined and the root cause of the problem is found without assigning blame to specific staff members, this is unnecessary. Essential changes can be made when fundamental causes of system or process faults are correctly identified. A consistent, multidisciplinary approach to root cause analysis that uses frameworks like the five whys to delve down until all issues and defects are revealed is a helpful tool. Although it is now necessary for the wake of sentinel events, the Root Cause Analysis may and should be applied to all mistake causes, including near misses.
Kohn, L. T., Corrigan, J., Donaldson, M. S., & Institute of Medicine (U.S.). Committee on Quality of Health Care in America. (2000). To err is human : building a safer health system. National Academy Press. books.nap.edu/books/0309068371/html/index.html
Leape, L. L., Brennan, T. A., Laird, N., Lawthers, A. G., Localio, A. R., Barnes, B. A., Hebert, L., Newhouse, J. P., Weiler, P. C., & Hiatt, H. (1991). The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med, 324(6), 377-384. doi.org/10.1056/NEJM199102073240605
Martinez, W., Lehmann, L. S., Hu, Y. Y., Desai, S. P., & Shapiro, J. (2017). Processes for Identifying and Reviewing Adverse Events and Near Misses at an Academic Medical Center. Jt Comm J Qual Patient Saf, 43(1), 5-15. doi.org/10.1016/j.jcjq.2016.11.001
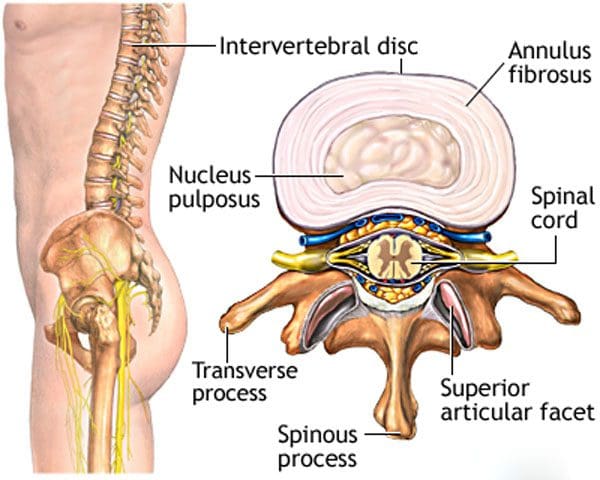
For individuals who are dealing with back pain and problems, could knowing how to improve and maintain intervertebral disc health help alleviate symptoms?
Intervertebral Disc Health
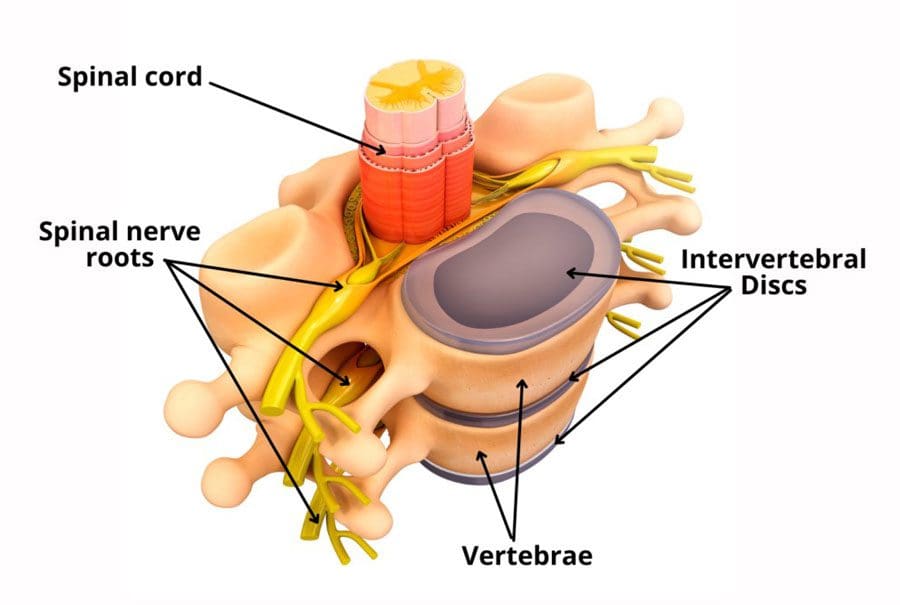
The spinal column comprises 24 movable bones and 33 bones called vertebrae. The vertebral bones are stacked on top of each other. The intervertebral disc is the cushioning substance between the adjacent bones. (Dartmouth. 2008)
Бонс
The vertebral bones are small and round in an area called the vertebral body. In the back is a bony ring from which protrusions extend and arches and pathways are formed. Each structure has one or more purposes and includes: (Waxenbaum JA, Reddy V, Williams C, et al., 2023)
Stabilizing the spine.
Providing a space for the connective tissue and back muscles to attach.
Providing a tunnel for the spinal cord to pass through cleanly.
Providing a space where nerves exit and branch out to all areas of the body.
Сохтори
The intervertebral disc is the cushioning that sits between the vertebrae. The design of the spine allows it to move in various directions:
Flexion or bending
Extension or arching
Tilting and rotation or twisting.
Powerful forces act upon and influence the spinal column to produce these movements. The intervertebral disc absorbs shock during movement and protects the vertebrae and spinal cord from injury and/or trauma.
Қобилият
On the outside, strong woven fiber tissues form an area called the annulus fibrosis. The annulus fibrosis contains and protects the softer gel substance in the center, the nucleus pulposus. (Y.S. Nosikova et al., 2012) The nucleus pulposis provides shock absorption, flexibility, and pliability, especially under pressure during spinal movement.
Механика
The nucleus pulposus is a soft gel substance located in the center of the disc that allows elasticity and flexibility under stress forces to absorb compression. (Nedresky D, Reddy V, Singh G. 2024) The swivel action alters the tilt and rotation of the vertebra above and below, buffering the effects of spinal motion. The discs swivel in response to the direction the spine moves. The nucleus pulposus is made mostly of water, which moves in and out through small pores, acting as byways between the vertebra and disc bone. Body positions that load the spine, like sitting and standing, push the water out of the disc. Lying down on the back or in a supine position facilitates water restoration into the disc. As the body ages, the discs lose water/хушк кардан, leading to disc degeneration. The intervertebral disc has no blood supply, which means that for a disc to receive necessary nutrition and for waste removal, it must rely on water circulation to stay healthy.
Нигоҳубин
Some ways of maintaining intervertebral disc health include:
Paying attention to posture.
Changing positions frequently throughout the day.
Exercising and moving around.
Applying correct body mechanics to physical activities.
Sleeping on a supportive mattress.
Нӯшидани оби зиёд.
Eating healthy.
Нигоҳ доштани вазни солим.
Drinking alcohol in moderation.
Даст кашидан аз тамокукашӣ.
At Injury Medical Chiropractic and Functional Medicine Clinic, we treat injuries and chronic pain syndromes by improving an individual’s ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. Our chiropractic team, care plans, and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Acupuncture, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Beyond the Surface: Understanding the Effects of Personal Injury
Waxenbaum, J. A., Reddy, V., Williams, C., & Futterman, B. (2024). Anatomy, Back, Lumbar Vertebrae. In StatPearls. www.ncbi.nlm.nih.gov/pubmed/29083618
Nosikova, Y. S., Santerre, J. P., Grynpas, M., Gibson, G., & Kandel, R. A. (2012). Characterization of the annulus fibrosus-vertebral body interface: identification of new structural features. Journal of anatomy, 221(6), 577–589. doi.org/10.1111/j.1469-7580.2012.01537.x
Барои шахсоне, ки мушкилоти узвҳои мушакӣ ва аломатҳои дардро аз сар мегузаронанд, метавонанд дар бораи биомеханика ва чӣ гуна он ба ҳаракат, тарбияи ҷисмонӣ ва иҷроиш, кӯмак дар табобат ва пешгирии ҷароҳатҳо омӯзанд?
Биомеханика
Биомеханика тамоми шаклҳои ҳаёт ва кори механикии онҳоро меомӯзад. Бисёриҳо дар бораи биомеханика дар варзиш ва иҷрои варзиш фикр мекунанд, аммо биомеханика ба эҷод ва такмил додани технологияҳо, таҷҳизот ва усулҳои барқарорсозии ҷароҳатҳо кӯмак мекунад. (Тунг-Ву Лу, Чу-Фен Чанг 2012) Олимон, духтурони тибби варзишӣ, физиотерапевтҳо, хиропракторҳо ва мутахассисони кондитсионер биомеханикаро барои кӯмак ба таҳияи протоколҳо ва усулҳои таълимӣ барои беҳтар кардани натиҷаҳои табобат истифода мебаранд.
Ҳаракати бадан
Биомеханика ҳаракати баданро меомӯзад, аз он ҷумла чӣ гуна мушакҳо, устухонҳо, пайҳоҳо ва пайвандҳо якҷоя кор мекунанд, хусусан вақте ки ҳаракат оптималӣ ё дуруст нест. Он як қисми соҳаи васеътари кинезиология мебошад, ки махсусан ба механикаи ҳаракат ва таҳлили он, ки чӣ гуна ҳама қисмҳои алоҳидаи бадан якҷоя кор мекунанд, то ҳаракатҳои варзишӣ ва муқаррариро ташкил медиҳанд. (Хосе М Вилар ва дигарон, 2013) Биомеханика дар бар мегирад:
Сохтори устухонҳо ва мушакҳо.
Қобилияти ҳаракат.
Механикаи гардиши хун, функсияи гурда ва дигар вазифаҳо.
Биомеханикаи варзишӣ ҳаракатро дар машқ, машқ ва варзиш меомӯзад, ки физика ва қонунҳои механикаро дар бар мегирад. Масалан, биомеханикаи машқҳои мушаххас ба инҳо назар мекунад:
Мавқеи бадан.
Ҳаракати пойҳо, зонуҳо, пушт, китфҳо ва дастҳо.
Донистани шаклҳои дурусти ҳаракат барои беҳтар кардани машқҳо ҳангоми пешгирии ҷароҳатҳо, ислоҳи хатогиҳои шакл, огоҳ кардани протоколҳои омӯзишӣ ва баланд бардоштани натиҷаҳои мусбӣ кӯмак мекунад. Фаҳмидани он ки чӣ тавр бадан ҳаракат мекунад ва чаро он чӣ гуна ҳаракат мекунад, ба мутахассисони соҳаи тиб кӯмак мекунад, ки ҷароҳатҳоро пешгирӣ ва табобат кунанд, нишонаҳои дардро сабук кунанд ва корҳоро беҳтар кунанд.
Таҷҳизот
Биомеханика дар таҳияи таҷҳизоти ҷисмонӣ ва варзишӣ барои беҳтар кардани кор истифода мешавад. Масалан, пойафзол метавонад барои иҷрои беҳтарин барои скейтбордист, давандаи масофаи дур ё футболбоз тарҳрезӣ шавад. Бо ин мақсад сатҳи бозӣ низ омӯхта мешавад, масалан, чӣ гуна сахтии сатҳи майдони сунъӣ ба нишондиҳандаҳои варзишӣ таъсир мерасонад. (Хосе И. Приего-Кесада 2021)
Масалан, фаъолсозии мушакҳо дар велосипедронӣ бо истифода аз электромиография ва кинематика чен карда мешавад, ки ба муҳаққиқон дар таҳлили омилҳое, ба монанди мавқеъ, ҷузъҳо ё шиддатнокии машқ, ки ба фаъолсозӣ таъсир мерасонанд, кӯмак мекунад. (Хосе И. Приего-Кесада 2021)
Мушкилот
Дар биомеханика ҳаракатҳои бадан аз мавқеъгирии анатомӣ ишора мешаванд:
Рост истода, бо нигоҳи рост ба пеш
Дастҳо дар паҳлӯҳо
Дастҳо ба пеш нигаронида шудаанд
Пойҳо каме дур, ангуштони по ба пеш.
Се ҳавопаймои анатомӣ иборатанд аз:
Сагиттал - медиан - Тақсим кардани бадан ба нимаи рост ва чап ҳамвори сагиталӣ/медианӣ мебошад. Флексия ва васеъшавӣ дар ҳамвори сагиталӣ ба амал меоянд.
Фронтал - Ҳавопаймои фронталӣ баданро ба паҳлӯҳои пеш ва қафо тақсим мекунад, аммо инчунин рабудан ё дур кардани узвро аз марказ ва аддуксия ё ҳаракат додани даст ба самти марказ дар ҳамвории фронталӣ дар бар мегирад.
Гузариш - уфуқӣ. – Қисмҳои болоӣ ва поёнии бадан бо ҳамвории уфуқӣ/кӯлӣ ҷудо мешаванд. Дар ин ҷо ҳаракатҳои гардиш ба амал меоянд. (Шӯрои Амрико оид ба машқ 2017)
Ҳаракати бадан дар ҳар се ҳавопаймо бо фаъолияти ҳаррӯза сурат мегирад. Ин аст, ки чаро иҷрои машқҳо дар ҳар як ҳамвории ҳаракат барои эҷоди қувват, функсия ва устуворӣ тавсия дода мешавад.
Tools
Барои омӯзиши биомеханика асбобҳои гуногун истифода мешаванд. Таҳқиқот одатан бо истифода аз дастгоҳе, ки бо номи электромиография ё сенсорҳои EMG маъруфанд, анҷом дода мешаванд. Дар давоми машқҳои санҷишӣ сенсорҳо ба пӯст гузошта мешаванд ва миқдор ва дараҷаи фаъолшавии нахи мушакҳоро дар мушакҳои муайян чен мекунанд. EMGs метавонанд кӯмак расонанд:
Клодикатсия/таъмини неврогенӣ ва илтиҳоби асабҳои сутунмӯҳра метавонад боиси кашиш, дард ва/ё ҷилавгирӣ дар пушт, пойҳо, хипҳо ва думҳо гардад. (Мартин Ҷ. Вилби ва дигарон, 2009)
Агар сутунмӯҳра ҷалб карда шавад, он метавонад боиси он гардад миелопатия/фишори шадиди ҳароммағз, ки метавонад боиси карахтӣ, заифӣ ва мушкилоти мувозинат гардад. (Дон Шин Ким ва дигарон, 2014)
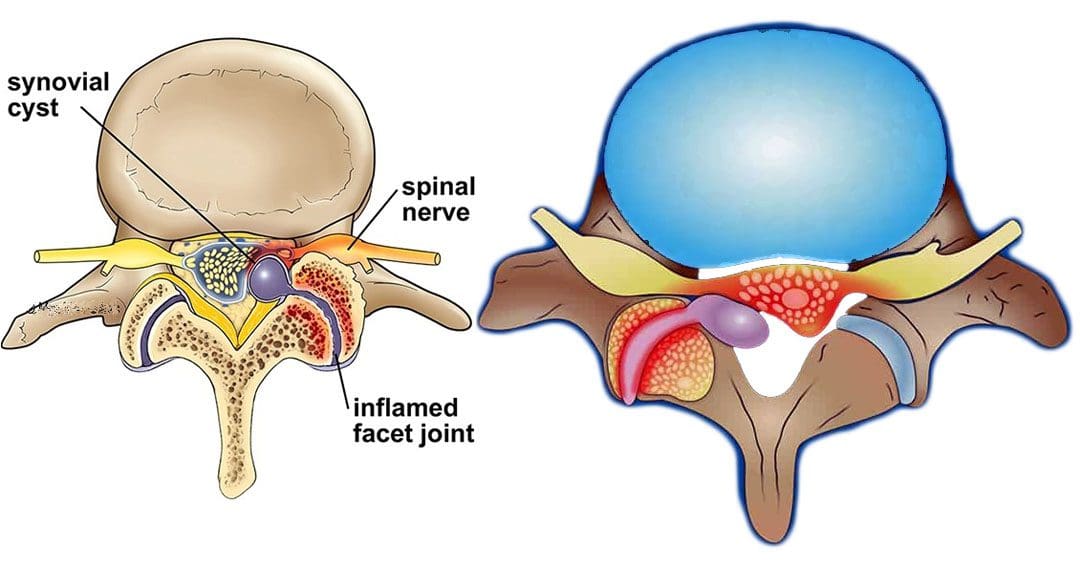
Аломатҳои марбут ба equina cauda, аз ҷумла мушкилоти рӯда ва/ё масона, заъфи пойҳо ва наркозҳои зин/гум кардани ҳиссиёт дар ронҳо, дандонҳо ва перинеум, метавонанд ба назар гиранд, аммо каманд, мисли кистаҳои синовиалӣ дар пушти миёна ва гардан. Агар кистаҳои синовиалӣ ва гарданаки бачадон инкишоф ёбанд, онҳо метавонанд аломатҳоеро ба монанди карахтӣ, карахтӣ, дард ё заъф дар минтақаи зарардида ба вуҷуд оранд.
Синдроми чапи боло як ҳолатест, ки дар он мушакҳои китфҳо, гардан ва сандуқҳо заиф ва танг мешаванд ва одатан аз машқ кардани мавқеи носолим ба вуҷуд меоянд. Аломатҳо одатан дар бар мегиранд:
Сахтии гардан ва эҳсоси кашидан.
Шиддати ҷоғ ва/ё тангӣ
Шиддати болоии пушти сар, набудани чандирӣ, сахтӣ ва дарди дарднок.
Дарди гардан, китф ва болои пушт.
Марди саркашӣ
Китфҳои мудаввар
Сутунмӯҳраи хамида
Синдроми салиб ва ҳолати болоӣ
Ҳолат ба ҳолати солим тавассути эҷод таъсир мерасонад мушакҳои номутаносиби байни пушти боло ва сандуқ.
Мушакҳои танги кӯтоҳи сандуқи болоии сина аз ҳад зиёд дароз мешаванд ва дар ҳолати нимпаҳншуда боқӣ мемонанд, ки мушакҳои қафоро кашида мегиранд.
Ин боиси кашидани мушакҳои пушт, китфҳо ва гардан мегардад.
Дар натиҷа пушт хамида, китфҳои пеш ва гардани барҷаста аст.
Институти миллии ихтилоли асаб ва инсулт. Дарди пушт.
Сидар-Синай. Дарди пушт ва гардан.
Геверс-Монторо, С., Провенчер, Б., Дескарро, М., Ортега де Мюес, А., ва Пиче, М. (2021). Самаранокии клиникӣ ва самаранокии манипуляцияи сутунмӯҳра барои дарди сутунмӯҳра. Сарҳадҳо дар таҳқиқоти дард (Лозанна, Швейтсария), 2, 765921. doi.org/10.3389/fpain.2021.765921
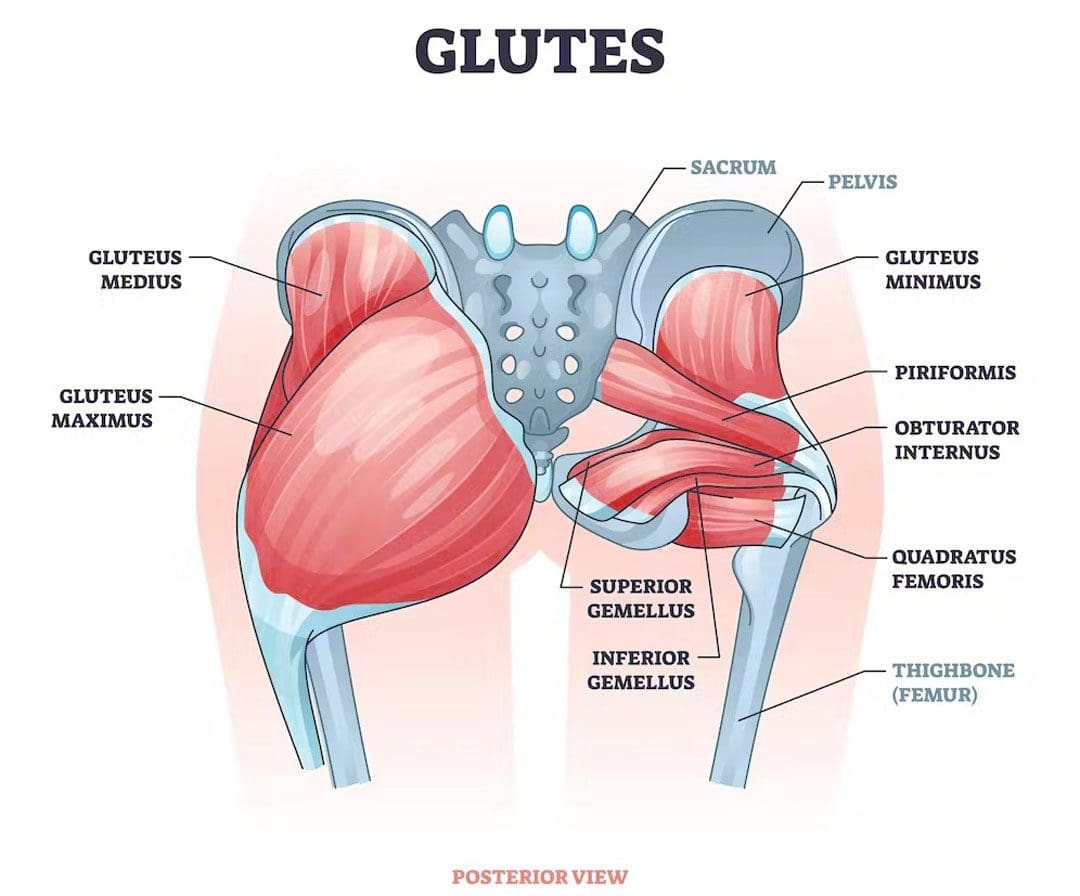
Мушакҳои gluteal/gluteal аз думҳо иборатанд. Онҳо як гурӯҳи мушакҳои пурқуввате мебошанд, ки аз се мушак иборатанд. Гluteus maximus, gluteus medius ва gluteus minimus. Мушакҳои glute ба қобилияти ҷисмонӣ ва ҳаракатҳои ҳаррӯза, ба монанди роҳ рафтан, истодан ва нишастан кӯмак мекунанд ва барои пешгирии осеби мушакҳои аслӣ, пушт, мушакҳои шикам ва дигар мушакҳо ва бофтаҳои пуштибон кӯмак мекунанд. Шахсони алоҳида метавонанд номутавозунии глютро инкишоф диҳанд, ки дар он як тараф бартарӣ пайдо мекунад ва аз тарафи дигар бештар фаъол мешавад ё баландтар аст. Нобаробарӣ, ки ҳал карда намешавад, метавонад ба мувозинати минбаъдаи мушакҳо, мушкилоти мавқеъ ва мушкилоти дард оварда расонад. Клиникаи тиббии хиропрактикӣ ва функсионалӣ метавонад нақшаи табобати инфиродиро барои рафъи нишонаҳо ва барқарор кардани ҳамоҳангӣ, мувозинат ва саломатӣ таҳия кунад.
Мувозинати мушакҳои glute
Glutes қавӣ, солим мусоидат суботи lumbopelvic ва ритми, маънои онро дорад, ки онҳо пушт ва коси камро дар ҳамоҳангии дуруст нигоҳ медоранд, то шиддатҳо ва ҷароҳатҳоро пешгирӣ кунанд. Нобаробарии глюта вақте рух медиҳад, ки як тарафи глутҳо калонтар, қавитар ё бештар бартарӣ доранд. Мувозинати глюта маъмул аст ва як қисми анатомияи муқаррарии инсон аст, зеро бадан комилан симметрӣ нест. Гузариш ва истифода бурдани тарафи бартаридошта ҳангоми гирифтани вазн ё гирифтани ашё муқаррарӣ аст, аз ин рӯ як тараф калонтар мешавад. Чӣ тавре ки шахс як даст, даст ва поро аз дигараш бартарӣ медиҳад, як паҳлӯи гулӯла метавонад сахттар кор кунад ва қавитар шавад.
Сабабҳо
Якчанд сабабҳои номутавозунии мушакҳои glute вуҷуд доранд, аз ҷумла:
Вариантҳои анатомӣ - Ҳар як шахс мушакҳои беназири шаклаш, нуқтаҳои пайвастшавӣ ва роҳҳои асаб дорад. Ин тафовутҳо метавонанд як тарафи гулӯлаҳоро бартарӣ ё қавитар кунанд.




 Қобилият
Қобилият